Breast Health
Breast Health
Breast Thermography is a painless, non-invasive, state of the art clinical test of physiology without any exposure to radiation and is used as part of an early detection program which gives women of all ages the opportunity to increase their chances of detecting breast disease at an early stage. It is particularly useful for women under 50 where mammography can be less effective due to dense breast tissue.
Thermography is also appropriate for women of all ages who, for many reasons, are unable to undergo routine mammography. Digital Infrared Thermal Imaging (DITI) is FDA-cleared as an adjunctive tool to primary screening. This test can provide a "clinical marker" for the doctor or mammographer that a specific area of the breast needs a particularly close examination.
DITI's role in breast cancer and other breast disorders is to help in early detection and monitoring of abnormal physiology and the establishment of risk factors for the development or existence of cancer.
When used with other procedures the best possible evaluation of breast health is made.
This quick and easy test starts with a review of a patient's medical history. The first DITI session provides the baseline of a patient's "thermal signature." Subsequent sessions assure that the patterns remain unchanged.
All thermograms (images) are kept securely on record. Once a stable thermal pattern is established, any changes can be detected during routine annual screenings.
(Source: Meditherm)
Breast Screening FAQ
Thermography or Digital Infrared Thermal Imaging offers the opportunity of earlier detection of breast disease than has been possible with breast self-examination, physician palpation or mammography alone.
Each individual has her own thermal pattern (normally symmetric) that is accurate and static throughout her lifetime. Any changes to her normal “thermal fingerprint” caused by early cell changes (pathology) will become increasingly apparent. Monitoring changes over periods of time with DITI is the most efficient means of identifying subjects who require further investigation.
DITI is a non-invasive test. There is no contact with the body of any kind, no radiation and the procedure is painless. The scanning system merely detects and records the infrared radiation that is emitting from the patient’s body.
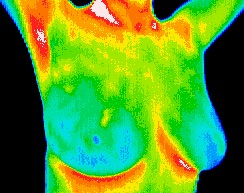
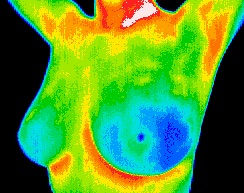
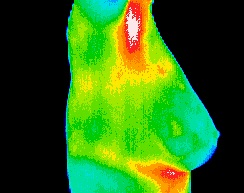
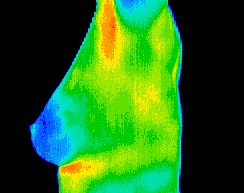
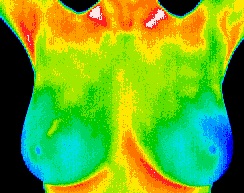
Utilizing sophisticated infrared technology and innovative computer software, thermal imaging technicians simply capture a digitized image of the breast in the form of an infrared thermogram, or heat picture.
Is cold stress testing of the breast necessary?
Cold Stressing Breasts and Why Don’t We Do It Anymore
A Position Paper and Discussion
By Peter Leando
Cold stress testing of the breast was performed on the assumption that thermography would identify angiogenesis and that angiogenesis could be correlated with the development and existence of breast cancer. This can be possible if a number of factors are present but there are too many variables that we now know make this an unreliable procedure. We don’t know at what stage angiogenesis begins but we do know that it does not continue throughout all stages of breast disease. No studies have been done to find out how long it takes for new (angiogenic) blood vessels to establish sympathetic fibers which then let the vessel behave like a normal vessel (contract when cold stressed) but even if we did have a better understanding of this physiology it would still not be a reliable test as many patients would undoubtedly fall outside of the window of detectable angiogenesis.
Considerations, the logic and philosophy of performing a cold stress test:
- If there are no suspicious thermal patterns to test, (negative thermogram) the test is not justified.
- If there are suspicious patterns (positive thermogram) then the patterns remain suspicious irrespective of the results of cold stress testing……. A cold stress test does not and should not affect the thermographic opinion and resulting report.
- A cold stress test might offer results relating to a particular suspicious pattern but if there is no way of correlating this information to a clinically valid or plausible rational to act on this information then the test is not justified in the first place.
- If a cold stress test is performed and the results are reported, this changes the status of the test and the report, both of which make claim to diagnostics and will carry the associated increase of liability and issues of scope of practice and medical licensure (practicing medicine without a license).
- The disservice to patients who suffer unnecessary mammography, biopsy, and other tests as a result of positive thermography generated by the attempt to produce diagnostic results from a single study is unacceptable.
- Reporting vascular change over extended periods of time by comparative analysis of thermal testing may be enhanced by the inclusion of a cold stress test if ordered specifically by a licensed physician who can integrate the results into decision making or a differential diagnosis. Historically, it was the way breast thermography was used with protocols that included cold stress testing (and the diagnostic claims that were made) which generated the criticism that thermographers still suffer from today. The accusations of unreliability and the clinical trial results showing false positives and false negatives were all generated by the protocols that included cold stress testing. Cold stress is a test of sympathetic function which has good utility in many areas of medicine and is the definitive diagnostic test for CRPS / RSD. These tests were used before it was tried in breast screening.
In the mid-eighties many people, including myself got excited by the potential offered by breast thermography performed with cold stressing. I was lucky enough to be working in France where the concept originated and I did a lot of cold stress thermography with a liquid nitrogen cooled NEC Sani and a Hues Aircraft Probeye, both of which were excellent cameras at the time. My own observations regarding the low rates of correlation between the results of cold stress tests and case histories and the growing evidence of false positives and false negatives led me to abandon cold stressing of breasts in the early nineties. I learned a more logical and more efficient approach which still relied on the detection of changes in the breast over time but was far more objective and reliable.
We have advanced significantly in our understanding of physiology and how thermography can be effectively used. No technology stands still, we expect science to advance, medical knowledge to improve and evolve and we have to be prepared to learn from experience….. both our own and others. I have no doubt that there will be ongoing advances in thermographic imaging and they may even include new forms of stress testing but the best way to move forward is to learn from experience and then look ahead rather than back.
First published August 2003 ACCT Thermology Times.
The Validity of Dynamic Stress Testing
Source: http://www.thermologyonline.org/Breast/breast_thermography_questions.html